Posterior Circulation Stroke: How Delays in Recognition and Escalation Become Catastrophic
- Terrance DeAngelo
- Feb 25
- 3 min read

Updated: Feb 27
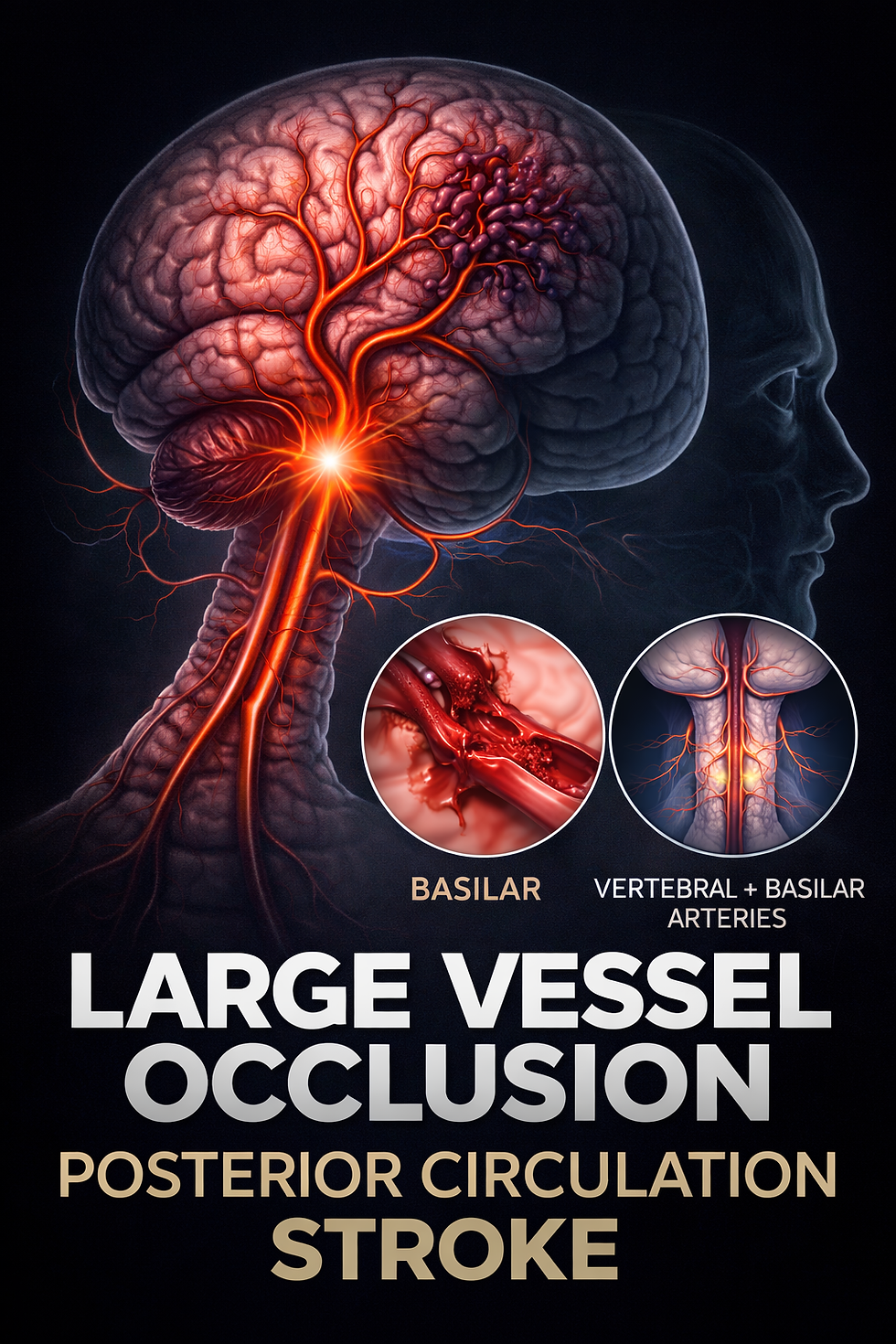
Posterior circulation strokes are among the most dangerous and frequently misdiagnosed forms of stroke. Unlike classic strokes involving facial droop or one-sided weakness, these events often present with subtle neurological symptoms and can deteriorate rapidly when escalation is delayed. Because they often involve the vertebral and basilar arteries supplying the brainstem and cerebellum, posterior strokes carry a high risk of sudden neurological decline, hydrocephalus, and death if not recognized and treated quickly.
Why Posterior Strokes Are Different
Posterior circulation strokes affect:
The brainstem
The cerebellum
Critical autonomic and coordination pathways
Symptoms often do not follow the typical stroke pattern and may include:
Severe dizziness or imbalance
Persistent vomiting
Slurred speech
Confusion
Difficulty swallowing
Visual changes
Gaze abnormalities
These presentations are easier to misinterpret, which can delay stroke-specific evaluation and escalation.
A Real Clinical Progression
In one documented case involving posterior circulation stroke, vascular imaging identified occlusion within the vertebral artery system early in the patient’s hospital course.
Despite this finding, the vascular abnormality was not initially treated as the cause of the patient’s evolving neurological deterioration. Over the hours that followed, the patient developed:
Persistent vomiting
Dysphagia and inability to tolerate intake
Confusion and cognitive changes
Progressive neurological decline
Severe hypertension
Clinical documentation reflected concern for vertebral artery occlusion and worsening neurological status. This type of progression is consistent with posterior circulation stroke deterioration.
When Stroke Protocols Exist but Escalation Breaks Down
Modern stroke systems are designed around speed and coordination. Stroke alert pathways are intended to mobilize emergency medicine, neurology, radiology, and nursing simultaneously so treatment decisions can be made without delay. These protocols emphasize:
Early recognition of stroke symptoms
Immediate neurologic assessment
Rapid imaging
Stroke-team activation
Coordinated escalation of care
They exist to reduce death and disability through time-sensitive intervention. When that escalation does not occur, the biological progression of stroke continues.
Large-Vessel Occlusion Is a Trigger for Action
Occlusion of the vertebral or basilar arteries represents a large-vessel stroke involving the posterior circulation. Within stroke systems of care, identification of large-vessel occlusion is not incidental. It is a trigger for:
urgent neurological reassessment
treatment planning
consideration of advanced intervention
transfer when higher-level stroke capability is required
Time targets for these decisions are measured in minutes.
The Point Where Neurology Becomes Neurosurgery
Cerebellar strokes introduce a mechanical danger inside the skull. As swelling increases:
The cerebellum expands within a fixed space
The fourth ventricle becomes compressed
Cerebrospinal fluid flow is obstructed
Hydrocephalus develops
Pressure builds around the brainstem
Herniation can follow
At this stage, neurosurgical intervention may include:
external ventricular drainage
decompressive surgery
But timing is critical. Once massive infarction and brainstem compression occur, recovery may no longer be possible.
Why These Cases Are Missed
Posterior strokes are more likely to be misdiagnosed because:
symptoms mimic vestibular or metabolic conditions
early imaging can appear normal
vertebral artery findings may be underestimated
deterioration may occur gradually before becoming severe
communication failures delay escalation
But the underlying physiology continues to evolve regardless of interpretation.
Clinical Pattern Seen in Posterior Stroke Cases
Posterior circulation stroke often follows a recognizable sequence:
Early vascular abnormality identified
Symptoms evolve over hours
Neurological status worsens
Escalation delayed or incomplete
Stroke progression becomes catastrophic
Stroke systems are designed to interrupt this progression. When escalation does not occur, the outcome can change rapidly.
Why This Matters
Posterior strokes are not static events. They are evolving neurological emergencies.
Understanding how these cases unfold helps explain:
why subtle symptoms require serious evaluation
why vascular imaging matters
why escalation cannot be delayed
why transfer decisions are time-sensitive
why neurosurgical involvement may become urgent
For patients and families across Pennsylvania these medical timelines can determine whether recovery is possible or whether injury becomes permanent.
Disclaimer:
This article is for educational and informational purposes only and does not constitute medical or legal advice. It is not a substitute for professional medical evaluation or treatment. If you believe you are experiencing a medical emergency, contact emergency services immediately.


Comments